
Ref No: 1990
Abstract:
Case of neuroendocrine:Carcinomas are becoming an increasing threat to everyone in our lives. Neuroendocrine tumors of the recto sigmoid colon are very rare and are often misinterpreted as rectal ulcers until they reach their last stage which is why it was very important to spread their awareness among people. This project was carried out by examining various cases of neuroendocrine tumors of the recto sigmoid colon and developing ways of coming up its provisional prognosis in lieu of its management and treatment.
Background:
We are presenting a rare case of neuroendocrine tumors at the recto sigmoid junction. Rectal neuroendocrine tumours usually are asymptomatic, and few present with symptoms of rectal bleeding, constipation, and tenesmus.
Introduction
Carcinoid tumors of the colon are extremely rare tumours, compromising<11 % of all carcinoid tumors and 1% of colonic neoplasms. Typically carcinoid tumors of the colon present in the 6th -7th decade of life during evaluation for anorexia, abdominal pain, and unintentional weight loss. Rectal carcinoids are usually asymptomatic and are discovered incidentally during proctoscopy, sigmoidoscopy or digital rectal examination. Patients who do have symptoms typically present with rectal pain, bleeding, or constipation. Most gastrointestinal neuroendocrine tumors are found in the appendix (50%), and ileum (30%).
Case Presentation:
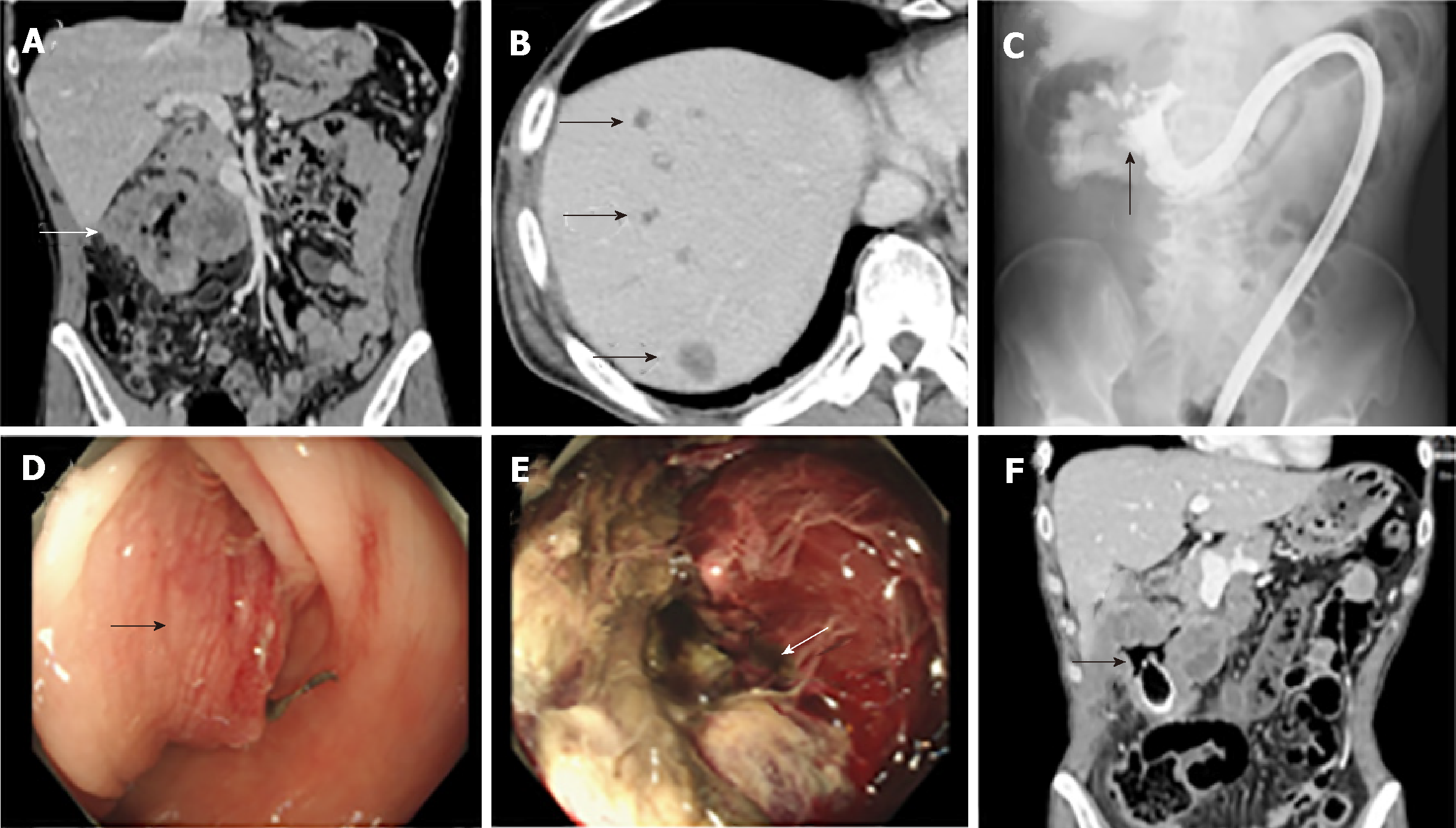
A 62-year-old gentleman known case of diabetes mellitus II, hypertension, dyslipidemia, bronchial asthma, presented with three months history of generalised fatigue, bleeding per-rectum, lose of appetite, and constipation. Physical examination was unremarkable. On PR exam internal piles found, no masses, or bleeding. Blood, mucus and recto sigmoid mass were seen on proctoscopy. Laboratory investigations showed hypochromic microcytic anemia, no leukocytosis, platelets were normal. Renal function tests were normal. CEA tumour marker pre-operatively was 5.28. Computed tomography diagnostic staging chest/abdomen/pelvis showed no evidence of distant metastasis, except for recto sigmoid mass. Patient underwent colonoscopy where semi-circumferential ulcerated mass with elevated edges of 12 cm to 16 cm from anal verge, covering recto-sigmoid junction was found. Biopsy taken showed inflammatory changes. Patient had undergone low anterior resection with diverting loop ileostomy. Biopsy result after surgical resection showed evidence of high-grade neuroendocrine carcinoma, large cell mass within the recto-sigmoid junction, staged pt3 pn1a pmx…..
Recent Comments